

Lately there were few people that came to see me with shoulder problems: restricted movement, bursitis, frozen, torn ligaments and muscles.
Some of them were even argumentative with me about their treatment, that I should be concerned just with their shoulder and leave along their back and pelvis.
So, I had to explain to best of my ability how imbalance in pelvic floor for example can influence/restrict the movements of the shoulder, how it all fit together in the body.
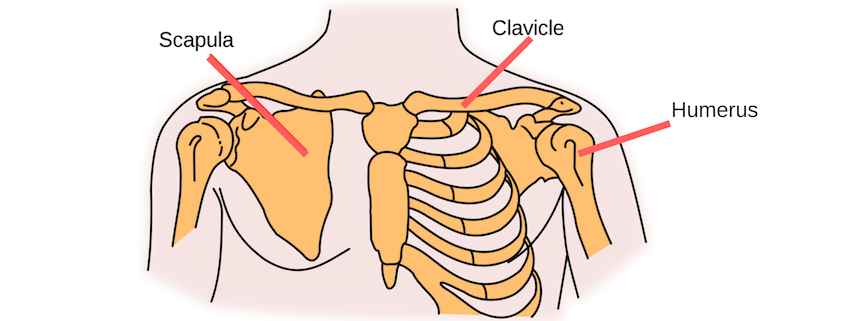
The shoulder joints
The shoulder is comprised of three bones – the clavicle (collarbone), the scapula (shoulder blade), and the humerus (upper arm bone) – as well as a range of muscles, ligaments and tendons.
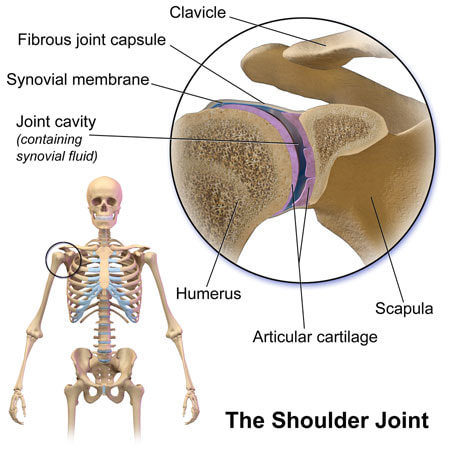
the glenohumeral joint
The main joint is the glenohumeral joint. This is where the head of the humerus attaches to the scapula at the glenoid cavity.
The joint is a type of ball and socket joint. The head of the humerus is the ball, with the glenoid cavity being the socket. The head of the humerus is much larger than the glenoid cavity, allowing a wide range of movement.
Cartilage covers the ends of the bones, and surrounding the joint space is a synovial membrane, allowing the shoulder to move. Around the joint space are many muscles (most notable are the rotator cuff muscles) and ligaments that help provide stability to the joint and make movement happy.
A number of bursae are located in the shoulder joint. Little fluid filled sacs, these bursae act as a cushion within the joint structure. Most important bursae are the subacromial and subscapular. The subscapular bursa lies between subscapularis tendon and the scapula. The subacromial bursa aims to reduce friction under the deltoid and allow free movement of the rotator cuff tendons. Inflammation of the subacromial bursa is a common cause of pain.
other parts of the shoulder
While the glenohumeral joint is seen as the main joint in the shoulder, a number of other joints and bony prominences have an influence on shoulder function.
The sternoclavicular (S/C) joint joins the clavicle to the sternum by a synovial joint. This is the one and only attachment point that connects the arm to the body.
At the other end of the clavicle is the acromioclavicular (A/C) joint. This joint attaches the clavicle to the scapula at the acromion (part of the scapula that forms the high point of the shoulder). This is also a synovial joint, acting like a pivot point to allow the arm to raise above the head.
Just below the acromioclavicular joint is a bony prominence worth noting – the coracoid process. This is the part of the scapula that you can feel at the front of your chest, below the collarbone and in from the glenohumeral joint. This part of the scapula is an attachment site for several muscles.
shoulder joint stability
The glenohumeral shoulder joint is one of the least stable joints in the body.
The socket is formed by the glenoid cavity of the scapula. This cavity is dish-shaped, and very shallow. This shallowness allows the arm to have a lot of mobility, but this also makes it easier to dislocate than most other joints in the body.
An analogy commonly used compares the humerus and the glenoid process to a golf ball and tee.
Key to shoulder stability are the rotator cuff muscles. These muscles surround the glenohumeral joint, attaching to the head of the humerus. When these muscles are at rest, they compress the head of the humerus into the glenoid cavity.
The glenoid labrum is a ridge to help deepen the cavity, create a seal with the head of the humerus and increase joint stability. Ligaments help to reinforce the joint capsule.
What Causes Frozen Shoulder?
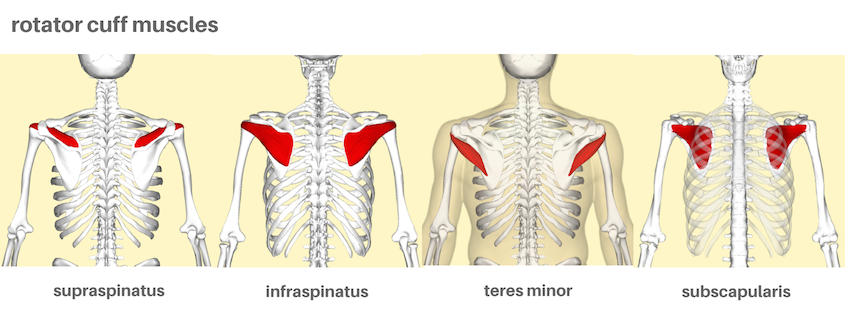
the muscles of the shoulder
The main group of muscles that stabilise the glenohumeral joint are known as the rotator cuff. The rotator cuff muscles join the scapula to the head of the humerus, forming a “cuff” at the shoulder joint. These hold the head of the humerus in the glenoid fossa during movement, preventing it from being pulled out of the joint by other muscles during movement. These muscles are key to stabilising the shoulder in the joint.
The rotator cuff group is not a single muscle. The muscles in this group are the supraspinatus, infraspinatus, teres minor and subscapularis.
– The supraspinatus joins the upper part of the scapula to the top of the humerus, and plays a part in the arm lifting up to the side.
– The infraspinatus and teres minor joins the lower part of the scapula to the top of the humerus. They play a part in lowering the arm to by the side, and pulling the shoulder backwards.
– The subscapularis is attached to the underside the scapula, sandwiched between the scapula and serratus anterior on the ribcage. It also attaches to the front of the humerus, playing a part in rolling the shoulder forward.
The deltoid muscle and teres major muscles are also part of the shoulder. This deltoid muscle is on the cap of the shoulder, with the glenohumeral joint underneath. The deltoid originates on the clavicle, and the acromion and spine of the scapula, inserting on the humerus. Teres major joins the lower point of the scapula to the upper part of the humerus.
These muscles are key to moving the arm and shoulder in all directions.
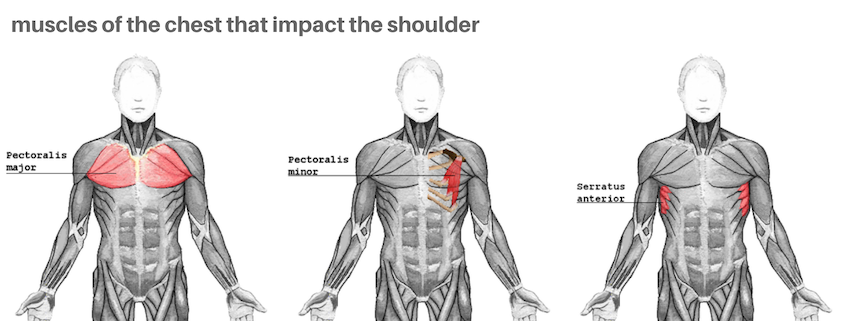
muscles in the chest impact the shoulder
With more experience as a Bowen Therapist, I started to see patterns in clients. I began to look deeper into what was going on, wanting to understand the shoulder more. I was initially surprised how many other muscles controlled the shoulder and it’s movement – muscles in the chest and in the back.
One thing that I often see with clients as they lie on their back is how rounded their shoulders are. Sometimes one, sometimes both. It’s usually muscles at the front of their body that cause this – not the actual muscles in the shoulder we spoke of earlier.
The powerful pectoralis major muscle in the chest, joins the sternum and part of the clavicle to the upper part of the humerus. We use this muscle to do all manner of movements when our are arms forward. But if this muscle becomes contracted and short, we see that shoulder(s) are often rounded as the pectorals pull the upper arm forward.
The pectoralis minor muscle lies under the pectoralis major. It attaches the corocoid process of the scapula with a number of ribs. When the pectoralis muscle is contracted and short, it pulls the scapula (and thus shoulder) out of good alignment. The scapula may be depressed (pulled down), abducted (pulled out) and downwardly rotated.
Serratus anterior is located under the arm, linking the medial (inner) edge of the scapula with a number of the ribs in the chest. This muscle is key to many scapula movements, and helps to fix the scapula in place against the ribcage. When this muscle is weak, the scapula is often see to be “winged” – sticking out of the back.
The sternocleidomastoid (SCM) attaches the temporal bone of the skull (behind the ear) with the sternum and clavicle. A muscle that controls the head and often pulls it forward, a tight SCM also impacts the shoulder indirectly by pulling on the clavicle.
Clients often feel their shoulders drop back and start to relax following a little work over the pectorals or their sternocleidomastoid.
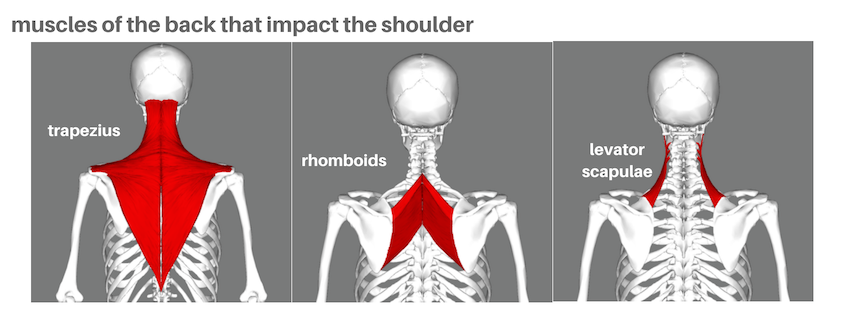
and muscles in the back impact the shoulder too
A number of muscles in the back have a clear influence on the position of the scapula, and thus the shoulder. Some are obvious, some less so.
The trapezius runs through the middle of the back, like a big wing connecting the spine (through the ribcage and neck to the occiput) to the clavicle and spine scapula. Different parts of the muscle have different impacts on the scapula – it may be pulled up or down, pulled in toward the spine, or cause the scapula to rotate. It’s a muscle that many people say feels like a rock (although, for many, it’s the levator scapulae that’s the rock).
The rhomboid muscles link the inner border of the scapula to the spine. These pull the scapulae toward the spine, can elevate the scapula, and play a part with downward rotation of the scapula (the scapula turns away from the neck toward the shoulder). The rhomboids are often blamed for feeling sore and “tight” – but the reality is that these are more often weak than strong. When these are weak, the scapulae are often very wide on the back – other muscles are to “blame” for them feeling tight !
Levator scapulae links the scapula with vertebrae of the cervical neck. These are often the muscles that feel very tight like rocks near the side of the neck. As well as controlling some neck movements, the levator scapulae elevate (ie raise) the scapula and rotate the shoulder blade away from the neck.
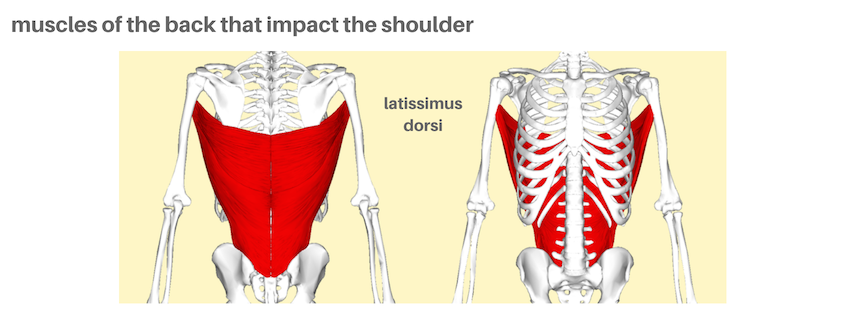
Latissimus dorsi is the broadest muscle of the back and not often thought of by many as a shoulder muscle. It originates on the pelvis’s iliac crest and lumbar (via the thoracolumbar aponeurosis), part of the thoracic spine and the lower tip of the scapula. Inserting on the upper part of the humerus at the front of the arm, it helps pull the arm down from overhead. It also pulls the arm into the body and pulls the shoulder forward.
Yes, you read that last part correctly – there’s a muscle connecting the pelvis to shoulder blade and the arms.
don’t forget the arms !
And just as the shoulder controls arm movement, the muscles of the arms impact the shoulder.
The biceps brachii are on the front part of the arm, linking the forearm to the scapula. Besides making the elbow bend and forearm supinate, the biceps also contributes to flexing the shoulder (raising the arm forward)
The triceps, on the back of the upper arm, also have one part (the long head) attaching to the scapula. This muscle plays a part in extending the shoulder (lowering the arm) and adducting (bringing the arm to the body)
The coracobrachialis is often known as the “armpit” muscle, deep under chest and other arm muscles. Attaching the forearm with the coracoid process of the scapula, it helps flex and adduct the shoulder.

the shoulder is at the mercy of the rest of the body
The most mobile joint in the body, the shoulder is made up of a few bones, held in place by many many muscles, tendons and ligaments.
The scapulae are the foundation of the shoulder joint. But without direct bony connection with the spine or the ribs, the scapula is held in place by the action of a range of muscles, as outlined earlier.
Any movement of your upper arm utilises your scapula in some way. Any weakness in the various muscles that connect to it will translate into weakness in the movement, leading to other muscles compensating. Balance of soft tissue is crucial for the scapula to maintain a neutral rest position, from where it can move to allow movement of the arm through the shoulder joint.
The muscles that hold the scapula in place are dictated by the position of the thoracic spine and rib cage. And the position of the thorax can influence and be influenced by the pelvis and head position.
If the body is tilted, twisted or out of balance, then the shoulders have very little chance of being in their correct position.
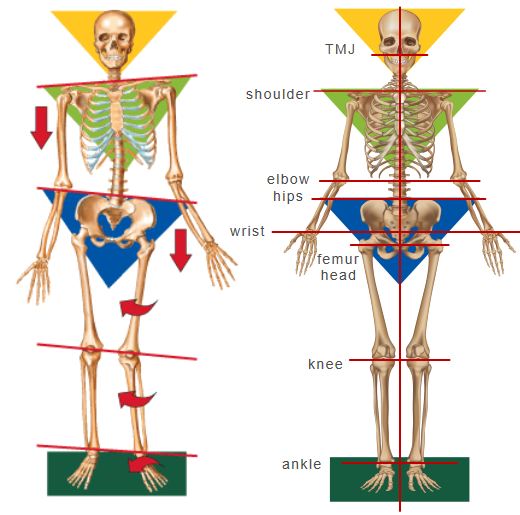
Helping only the muscles in the shoulder may give some relief, but that would be short lived. If the tension in the body that was pulling the shoulder out of its best neutral position wasn’t addressed, the shoulder will soon return to the compensated position. The arms “hang” off the body via the shoulders. How well they hang is directly determined by alignment of the torso. The shoulder is at the mercy of the rest of the body.

bowen therapy to help shoulders
It may surprise some people that when a client comes in with a shoulder problem, the shoulder is not the first area I look at. Or perhaps not a surprise after reading the previous section.
The shoulders are at the mercy of the rest of the body.
The main goal of most Bowen Therapists is to restore symmetry in the body. When the body has returned to symmetry, it’s then possible to feel what part of the shoulder’s musculature remains as problematic.
A Bowen Therapist will use Bowen moves on the length of the body, to help the spinal muscles and begin to restore balance in the total body. Using observation, touch and assessments, an experienced Bowen Therapist can pinpoint areas of primary restriction in the body. Specific moves can help those restricted areas and bring symmetry back to the body.
Only then will a Bowenwork practitioner move to the shoulders. A range of moves can help specific areas of restriction in the shoulder, the arm, the chest or the back.
how long will it take ?
For many, an initial level of improvement in shoulder mobility may come quickly, especially if the injury is acute.
However, some shoulder problems need time and patience. The body needs to become used to being aligned, before the shoulders can be in their best neutral position. Bursa that are irritated or frozen require time to recover and function properly again.
And for some, regular maintenance may be what’s needed. A client with torn rotator cuff muscles and a popped bicep is not only avoiding surgery with regular Bowen, but is swimming laps a few times a week again. Using Bowen to maintain balance in the torso, with attention to the muscles that tend to pull the shoulder, is keeping him working and exercising.
images
OpenStax College, via Wikimedia Commons
Anatomography, via Wikimedia Commons
Original by National Cancer Institute; SVG by Mysid [Public domain], via Wikimedia Commons
Blausen.com staff (2014). “Medical gallery of Blausen Medical 2014”. WikiJournal of Medicine 1 (2). DOI:10.15347/wjm/2014.010. ISSN 2002-4436. [CC BY 3.0 (https://creativecommons.org/licenses/by/3.0)], from Wikimedia Commons